Challenges to Transcatheter Closure of a Large Patent Ductus Arteriosus Using Internal Jugular Venous Access in Down Syndrome: A Case Report
- 1. Interventional Cardiologist, SKY Hospital & Research Centre Pvt. Ltd., India
- 2. Chief Cardiologist, SKY Hospital & Research Centre Pvt. Ltd., India
- 3. Academic Executive, SKY Hospital & Research Centre Pvt. Ltd., India
Abstract
Device closure of patent ductus arteriosus (PDA) via femoral vein is the commonly used transcatheter closure procedure, which is safe and effective. The internal jugular vein is not a typical vascular access for the device closure of PDA. Interrupted Inferior Vena Cava (IVC) acts challenges for PDA device closure. We report a case in which a large PDA was closed with device using transjugular venous approach. The transjugular route for device closure of patent ductus arteriosus is a viable effective and safe alternative route to conventional femoral venous access when the later route cannot be achieved due to various reasons.
Keywords
• Transcatheter closure
• Patent ductus arteriosus
• Internal jugular venous access
• Down syndrome
CITATION
Yadave R, Lairikyengbam SKS, Devi MA (2024) Challenges to Transcatheter Closure of a Large Patent Ductus Arteriosus Using Internal Jugular Venous Access in Down Syndrome: A Case Report. J Cardiol Clin Res. 12(1): 1198.
ABBREVIATIONS
PAH: Pulmonary Arterial Hypertension; PASP: Pulmonary Arterial Systolic Pressure; PDA: Patent Ductus Arteriosus; IVC: Inferior Vena Cava
INTRODUCTION
Device closure is an established method for treatment of PDA [1]. Mostly femoral venous access is used for the procedure. However, this route is not always possible due to obstruction or interruption of femoral vein or inferior vena cava. The other alternative means is transjugular route. There are only few case reports of transcatheter closure of PDA via internal jugular vein in children published in English medical literature. Patent ductus arteriosus is a common congenital heart defect accounting to 5-10% of all congenital heart diseases [2]. Trans-catheter occlusion of the PDA is nowadays considered to be a safe and effective method [3,4].
CASE REPORT
A four years and six months old girl with Down Syndrome weighing only 10 kg presented with a chief complaint of dry cough for 3 days. She had continuous murmur on clinical examination. An Echocardiographic examination revealed a large PDA (7.0 mm) with left to right shunt, severe PAH (PASP = 70 mm Hg), dilated left atrium (z- score + 4.60) and left ventricle (z-score + 4.40) with left ventricle (z-score + 4.40) with preserved left ventricular and right ventricular function (LVEF=76.6%). An Electrocardiogram revealed sinus rhythm with left & right ventricular hypertrophy and borderline prolonged QT interval. Chest X–ray showed cardiomegaly. This large PDA with dilated left ventricle with severe pulmonary hypertension had to be closed as early as possible either surgically or with device to save her life. Parents opted for non-operative device closure. An aortogram via right femoral artery confirmed a large PDA (7 mm) (Figure 1).
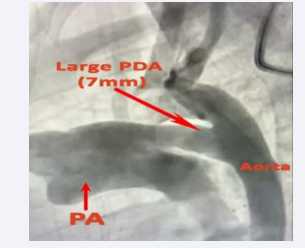
Figure 1: Fluoroscopic image showing large PDA of 7mm.
Femoral venous access on both sides could not be achieved despite ultrasound guidance due probably to Down Syndrome related venous anomaly. Transjugular approach was therefore chosen for the implantation of the PDA device.
A Cook extra stiff wire and a 8F Amplatzer sheath were used to cross the defect and placed in the descending aorta (Figure 2).
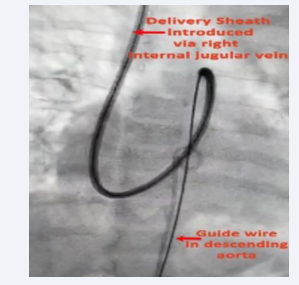
Figure 2: Fluoroscopic image showing delivery sheath introduced via right internal jugular vein and guide wire in descending aorta.
A Life-tech PDA device (14/12) was deployed leading to the complete closure of the PDA (Figures 3-5).
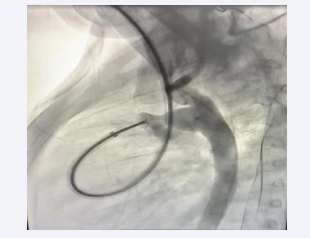
Figure 3: The aortogram via femoral artery checking the position of PDA device.
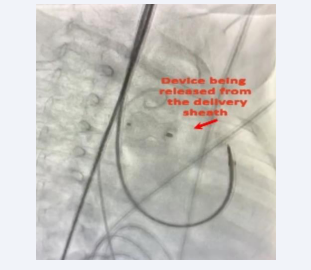
Figure 4: Fluoroscopic image showing device being released from the delivery sheath.

Figure 5: Final check with aortogram showing complete closure of PDA with device.
The procedure was performed under general anaesthesia and under Fluoroscopic screening and transthoracic Echocardiography guidance. Device was released from the delivery sheath checking that it was properly implanted (Figure 4).
DISCUSSION
Femoral venous access for PDA device closure is considered as the standard vascular access procedure in pediatric and adult patients due to the low incidence of associated complications and easier manipulation of the device compared to other access routes. However, this may not always be possible if there is any interruption or obstruction in the route of femoral vein or inferior vena cava. In our case, the femoral venous access on both sides could not be achieved despite ultrasound guidance due probably to Down Syndrome related to venous anomaly. Irrespective of the symptomatic status, clinically audible PDAs are closed surgically or through videoscopic assisted minimally invasive technique or percutaneously using coils or devices [5- 10] (Figure 6 and Video 1).
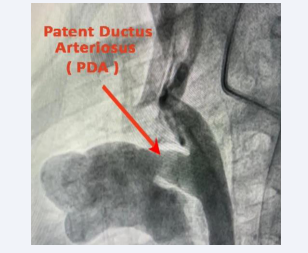
Figure 6: Video clip of PDA Device closure through jugular vein.
With the advent of Duct occluder, almost all the PDAs beyond neonatal period and early infancy are closed with the transcatheter technique [11]. The difficulties associated with the transjugular approach include placing a large sheath in the jugular vein, directing the catheter through the defect, manipulating to cross the defect, and placing a catheter or guide wire in the descending thoracic aorta. Percutaneous closure of the patent ductus arteriosus (PDA), in patients with interrupted inferior vena cava poses a technical challenge [12]. In our case, there was no undue difficulty or complication bigger size PDA device (14/12), had to be used. The ECHO done just before discharge from hospital showed the device in situ with complete closure of the PDA. The PASP came down from 70.0 mmHg to 45.0 mmHg. His case report shows the usefulness of the internal jugular vein as an alternative route for device closure of PDA in patients when femoral venous access is not possible.
CONCLUSION
The transjugular route for device closure of patent ductus arteriosus is a viable effective and safe alternative route to conventional femoral venous access when the later route cannot be achieved due to various reasons
REFERENCES
- Aggarwal N, Agarwal M, Joshi R, Joshi RK. Device closure of patent ductus arteriosus in interrupted inferior vena cava. Ind Heart J. 2015; 67.
- Schneider DJ, Moore JW. Patent ductus arteriosus. Circulation. 2006; 114: 1873-1882.
- Wang JK, Wu MH, Hwang JJ, Chiang FT, Lin MT, Lue HC. Transcatheter closure of moderate to large patent ductus arteriosus with the Amplatzer duct occluder. Catheter Cardiovasc Interv. 2007; 69: 572- 578.
- Baruteau AE, Hascoët S, Baruteau J, Boudjemline Y, Lambert V, Angel CY, et al. Transcatheter closure of patent ductus arteriosus: past, present and future. Arch Cardiovasc Dis. 2014; 107: 122-132.
- Rashkind WJ, Mullins CE, Hellenbrand WE, Tait MA. Non-surgical closure of patent ductus arteriosus: Clinical application of the Rashkind PDA occluder system. Circulation. 1987; 75: 583-592.
- Verin VE, Saveliev VS, Kolody SM, Prokubovski VI. Results of transcatheter closure of the patent ductus arteriosus with the Botalloocluder. J Am Coll Cardiol. 1993; 22: 1509-1514.
- Hijazi ZM, Geggel RL. Results of anterograde multiple transcatheter of patent ductus arteriosus using single or Gianturco coils. J Am Coll Cardiol. 1994; 74: 925-929.
- Rao PS, Kim SH, Choi JY, Rey C, Haddad J, Marcon F, et al. Follow-up results of transvenous occlusion of patent ductus arteriosus with the buttoned device. J Am Coll Cardiol. 1999; 33: 820-826.
- Porstmann W, Wierny L, Warnke H. Closure of the persistent ductus arteriosus without thoracotomy. Ger Med Mon. 1967; 12: 259-261.
- Gross RE, Hubbard JP. Surgical ligation of a patent ductus arteriosus.A report of first successful case. JAMA. 1939; 112: 72-31.
- Masura J, Walsh KP, Thanopoulos B, Chan C, Bass J, Goussous Y, et al. Catheter closure of moderate to large sized patent ducts arteriosus using the new Amplatzer duct occluder: Immediate and short-term results. J Am Coll Cardiol. 1998; 31: 878-878.
- Jawahirani Anil. Percutaneous closure of patent ductus arteriosus via internal jugular vein in-patient with interrupted inferior vena cava. Ind Heart J Interven. 2018; 1: 56.







































































































































{kind=link}